Reprinted from :
THE RAJ ASTHAN MEDICAL JOURNAL
Vol. XIX, No. I, January 1980
Clinical Trial of Aloes Compound* in
Cases of Dysmenorrhoea
Navratan Bafna **
Madhu Mehta ***
Introduction
‘Dysmenorrhoea’ literally means difficult menstruation. But in practice, the term is applied to painful menstruation which disables the patient from doing her normal work and duties and it may last from a few hours to a few days. Dysmenorrhoea may be spasmodic (primary, intrinsic, essential, idiopathic) or congestive (secondary, extrinsic, acquired) or rarely it may be combined (spasmodic and congestive). Dysmenorrhoea may be seen in both unmarried and married women. It may be present in nulliparous and parous women. It may be present from the time of menarche or it may occur after a few years of normal, painless menstruation. Dysmenorrhoea may occur in those having normal periods and normal flow while in some dysmenorrhoea may be associated with irregular scanty period s. Added to these, psychological factors of the patient who generally comes with her well-meaning but over-anxious mother, aggravate the condition, as these decrease the patient’s threshold to menstrual pain. When omnibus measures of bed rest, analgesics, antispasmodics, sedatives, hormones, etc. do not relieve the condition, the treating physician feels helpless. If the girl is unmarried, she has advised marriage with the hope that this may solve the problem. If the woman is already married, she is advised to wait till she becomes pregnant and begets a child, when dysmenorrhoea will disappear. The waiting pregnancy may not take place, because dysmenorrhoea itself is a contributory factor in some cases of sterility. Also, dysmenorrhoea is often associated with scanty, irregular periods which adds to primary sterility further. So pregnancy and childbirth are not a predictable or practical solution for dysmenorrhoea. Neither dysmenorrhoea is confined to women who have no children. Some patients of dysmenorrhoea are parous women. When medicines fail, the treating physician thinks of dilatation of the cervix. In unmarried girls, this is best avoided. In married women dilatation of the cervix is not a permanent cure of dysmenorrhoea. It is a hopeful measure. We must not forget that facilities for surgical measures even where indicated are mostly confined to well developed urban areas.
Aloes Compound (Alarsin) With this predicament and with no specific treatment for dysmenorrhoea before us, the current treatment being empirical, unpredictable and unsatisfactory, our thoughts went back to the days when Aloes was extensively used in cases of dysmenorrhoea in the form of pelvis aloes or pills aloes et ferri . While in search of a suitable aloes preparation, we came across the marketed product Aloes Compound (Alarsin). So we reviewed the literature on Aloes (Alarsin) Deshpande ( 1962) was the first to report on the “Use of Aloes Compound in irregular and scanty menstruation ” Balsara (1966), Jhaveri et al (1972), Mukherjee & Mukherjee (1972) Shah (1977) all reported successful use of Aloes Compound in cases of sterility associated with scanty, irregular menstruation. Gupta (1972), Rajasekharan (1975), Ramani Sivaraman (1976), Samanerkar (1977), conducted trials with Aloes Compound in cases of sterility. Mehta (1966) had tried Aloes Compound in lactational amenorrhoea. Bhatia (1971) had successfully used Aloes Compound in cases of dysmenorrhoea. This review of the literature on Aloes Compound encouraged us to try this drug in our own hospital on cases of dysmenorrhea.
Composition and actions of Aloes Compound (Alarsin)
Each tablet of Aloes Compound has the following composition :
|
Aloes Indica |
70 mg |
| Hira Bol (Balsamo- dendron Myrrha) | 70 mg |
| Hira Bol (Balsamo- dendron Myrrha) | 30 mg |
| Manjishta (Rubia cordifolia) | 35 mg |
| Hurmal (Pegunum harmala) | 35 mg |
| Kasis (Ferri sulphas) | 30 mg |
| Jeevanti (Leptadenia reticulata) | 30 mg |
The manufacturers have described that this combination regulates menstrual periods, improves fertility index reduces obesity and improves general health. Its indications are given as useful in amenorrhoea irregular, scanty menstruation, dysmenorrhoea primary or secondary sterility.
Material & Method
For the purpose of this clinical trial, 100 cases suffering from dysmenorrhoea were taken at random from the out patient department of the State Zenana Hospital, Jaipur, during l ½ years of 1977-78. Each patient was treated for four menstural cycles. However, out of 100 cases, complete follow-µp for the duration of clinical trial was possible only in 75 cases. As such t he final stud y could be done only on these 75 cases. Those found with organic causes were excluded from t he study.
Dosage of Aloes compound I Regimen : Aloes compound was started in all the 75 cases, in a dose of 2 tabs three times a day, five days before the expected date of menstruation. They were asked to take till the first day of menstruation . This was repeated every month for four menstural cycles, as this was the duration of the clinical trial.
II Regimen : Those cases of dysmenorrhoea associated with irregular, scanty menstruation and other menstrual disorders, were asked to take Aloes Compound 2 tabs. three times a day continuously, t hat is during and after menstruation, till their menstrual cycle became normal, when they were asked to follow I Regimen. In case the menstrual pattern did not become com pletely normal they were asked to continue 11 Regimen till the end of the clinical trial.
Aloes Compound was stopped immediately pregnancy was suspected
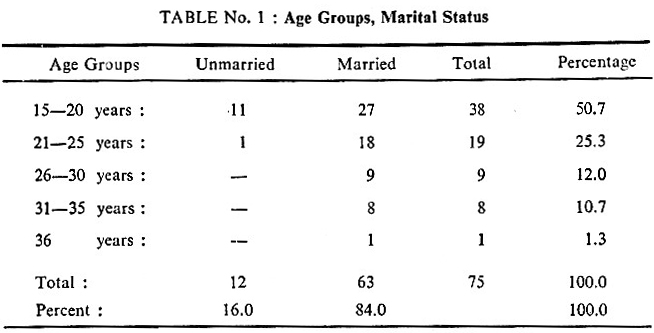
Age groups & marital status Among the 75 cases of dysmenorrhoea under study, 12 cases were unmarried and 63 cases were married. The largest number of cases, namely 38 (50.7) were in the age group of 15-20 years . On the whole, 76 0 were in the age groups 15-25 years. The details are given in Table I.
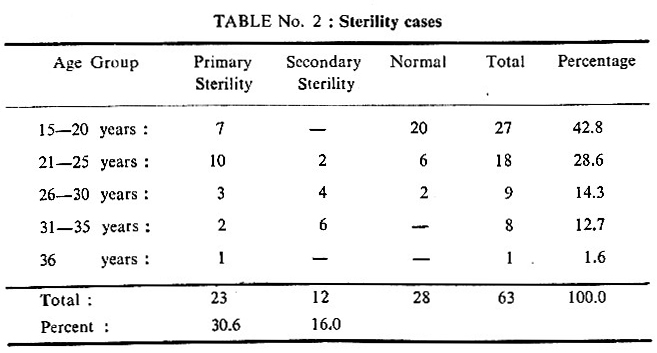
Sterility Among the 75 cases under study, 63 were married and among these 23 cases had primary sterility and 12 cases had secondary sterility. This shows that sterility is very high when dysmenorrhea is present (46.6%)· The details are given in table 2.
Menstrual Pattern Among the 75 patients under study, 27 patients (36%) bad normal menstrual pattern and the rest 48 patients had hypomenorrhea, oligomenorrhoea or scanty irregular menstruation. This shows that dysmenorrhoea is generally accompanied by menstrual disorders in about 64 of the cases. It denotes the importance of the drug to treat both dysmenorrhoea and menstrual disorders for the successful management of these cases. The details of the menstrual pattern are given in Table 3.
Table 3
Showing menstrual pattern
| Pattern | No of Cases | Percentage |
| Hypomenorrhoea | 9 | 12.0 |
| Oligomenorrhoea | 11 | 14.7 |
| Scanty Irregular periods | 28 | 37.3 |
| Normal Pattern | 27 | 36.0 |
| Total | 75 | 100.0 |
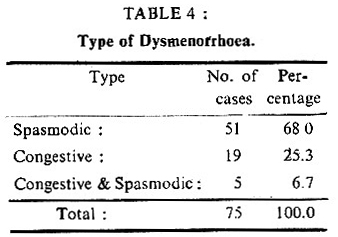
There were 51 patients with spasmodic dysmenorrhoea, 19 patients with congestive dysmenorrhoea, and 5 cases with the combined type (spasmodic and congestive). The details are given in Table 4.
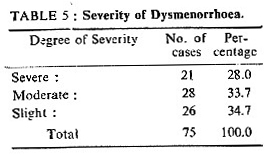
Severity of Dysmenorrhoea
The severity of dysmenorrhoea, being subjective, varies from person to person and may vary in different socio-economic communities, and it is well known that there is an increased thresh-hold to pain in lower socio-economic communities. As such, we have divided severity into three categories irrespective of the socio-economic group or environment. Severe dysmenorrhoea: where work was not possible; Moderate : where work was possible, with rest intervals, Slight : where work was possible though with a little discomfort. Most of the patients (65.3%) had either severe or moderately severe dysmenorrhoea. The details are given in Table 5.
Assodated Symptoms
Headache, maladies, constipation, weight-loss and fatigue were seen more commonly.
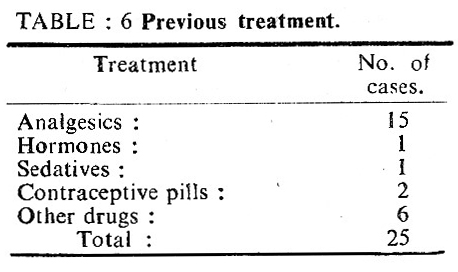
History of Previous Treatment
25 patients were treated with other drugs without relief before they came for treatment here. The details are in Table 6.
Assessment of Results
Results were assisted into well-demarcated categories of complete relief from dysmenorrhoea, moderate relief, and no relief. The results were evaluated monthly (after m.c.) for four months, which was the trial period. The treatment was stopped where the pregnancy was suspected.
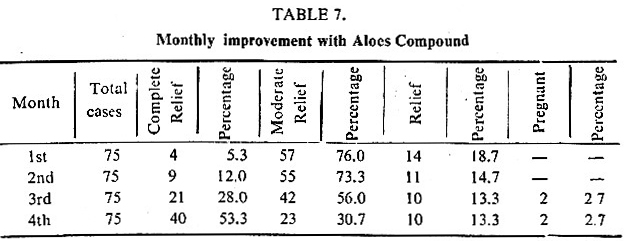
Monthly improvement with aloes compound
Improvement was assessed after each menstrual cycle. Complete relief, month wise was as follows: 1st month 4 cases; 2nd month: 5 cases; 3rd month : 12 cases; 4t h month : 19 cases. At the end of the clinical trial. a total of 40 patients had complete relief and 10 patients had no rel ief. In two cases pregnancy was suspected after three months of treatment and it was confirmed by the next month. The details are given in Table. 7
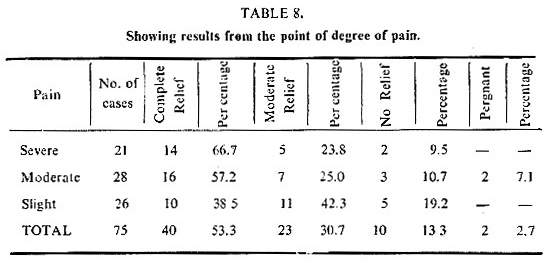
Results as to Severity of Dysmenorrhoea
At t he beginning of the clinical trial, there were 21 cases of severe dysmenorrhoea, 26 cases of moderate dysmenorrhoea, and 28 cases of slight dysmenorrhoea. Complete relief was as follows : 14 out of 21 cases of severe dysmenorrhoea , 16 out of 28 cases of moderate dysmenorrhoea and 10 out of 26 cases of slight dysmenorrhoea. Besides 2 cases from moderate group became pregnant. Drug response was comparatively better (66.7%) in severe cases. The details are given in Table. 8.
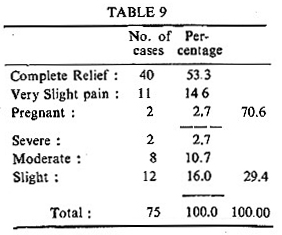
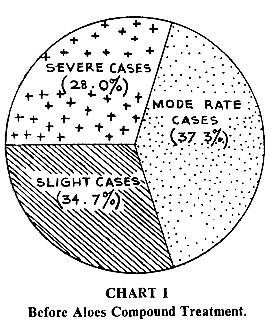
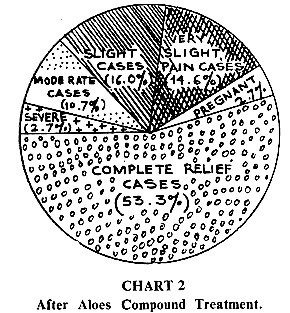
Position at the end or the Clinical Trial
While there is no difficulty about the categories of complete relief and no relief, moderate relief requires a little explanation, the meaning of which changes depending upon the category before the clinical trial. Moderate relief among the original moderate cases means slight pain. Moderate relief among the original slight cases means very slight pain,short of complete relief and this is an additional category after the clinical trial. On this basis, the final picture after the clinical trial was : Complete relief-40; Very slight pain- 11 ; Severe- 2; Moderate-8; Slight- 12; 2 patients became pregnant during treatment. One patient was married 8 months back and was treated for moderate dysrnenorrhoea. Another case had also moderate dysmenorrhoea, but was a case of primary sterility. The final picture of dysmenorrhoea at the end of the clinical trial is given in Table 9 and Charts I & II.
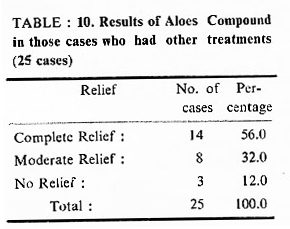
Results in those cases who had no relief with other drugs
There were 25 cases who were treated before with other drugs but without relief (Table 6). Out of these, after Aloes compound treatment, 14 cases (56.0% ) had complete relief, 8 cases (32.0%) had moderate relief and 3 cases ( l 2.0 % ) had no relief. On the whole, the response to Aloes compound in those cases that were previously treated unsucessfully with other drugs was quite satisfactory. The details are given
TABLE : 10. Results of Aloes Compound in those cases who had other treatments (25 cases)
Overall improvement with aloes compound
Those patients whose menstrual pattern was not normal showed normal or improved pattern of menstrual cycles.
Associated complaints like headache, malaise, fatigue became less. Those who showed a tendency to weight loss began to gain weight or atleast their weight loss was controlled. Those who had constipation showed improvement in their bowel movement. There was a sense of well· being in most of the cases irrespective of the degree of relief.
Over-all , the satisfactory improvement with the treatment of Aloes compound was 70.6% and t here was no relief in 29.4 % {Table 9).
Toxic or side effects
No side effects or toxic effects were observed with the use of Aloes compound.
Conclusion :
This clinical trial suggests that Aloes compound is useful in treating cases of dysmenorrhoea and associated symptoms. There was no difference in drug response whether it was spasmodic dysmenorrhoea or congestive dysmenorrhoea. Being non-hormonal, Aloes compound can safely be given even continuously for some months, where necessary.
Summary
75 cases of dysmenorrhoea were treated with Aloes compound for four menstrual cycles a t Jaipur, Zenana Hospital, during 1977-78. There were 12 unmarried women. 21 pa tients had severe dysmenorrhoea, 28 patients had moderate dysmenorrhoea and 26 patients had slight dysmenorrhoea . Check-up was made monthly after menstrual cycle. 53.3% had complete relief from dysmenorrhoea and 14.6% had very slight dysmenorrhoea, a total of 67.9% of satisfactory improvement. 2 cases became pregnant. No side effects were found with Aloes compound .
Acknowledgment
We are thankful to M r. R.K. Srivastava of Alarsin Pharmaceuticals, Bom bay for their cooperation.
REFERENCES
- Bhatia Gita, 111’re11t Medical Practice, 1971, 15,
- Chopra, R, N, Chopra, C., A Review of Work 011 Tndimz Me-medicinal Plants, published by I. C. M. R., 1955.
- Ghose, , Pharmacology, Materia Medica & Therapeutics, 20th Edition, 1 957.
- Nad karn i M., Indian Materia Medica, 1976, Popu la r Pra kasham, Bombay.
Masani M. (1956) :, Psychosomatic Problems in Gynaecolagy : Sir Kelil amatb Das Memorial Oration, 1966, Journal Obsietrics & Gynecology 17:2, 113.