DEKOFCYN:AN AYURVEDIC DRUG, IN THE RELIEF OF
COUGH IN CHILDREN
Dr. VASANT A. KHATAYV, M.D. (Bom.), D.C.H.,
Dr. Khatav’s Mother & Child Hospital, Arunoday Shopping Centre,
Borivli (West), Bombay-400 092.
INTRODUCTION DEKOFCYN: PROPERTIES
Cough is the most common complaint and Has anti-tussive, expectorant, demulcent,more so in children, who are prone to respirat- decongestant, anti-phlegmatic, anti-bacterial,ory diseases. Cough is a symptom of an under- anti-inflammatory, anti-allergic, haemostaticlying cause which may be due to bacterial or and general tonic properties. It is useful in theviral infections or allergy. The object of this management of cough, productive or non-pro-study was to assess whether Dekofcyn, an ductive, acute, chronic or resistant, wet or dry. ItAyurvedic product has beneficial action in re- increases body resistance by increasing the im-lieving cough as symptom with specific line of mune mechanism. Makes expectoration easy.treatment. (Waman Ganesh Desai, Nadkarni, Chopra).
COMPOSITION OF DEKOFCYN
Each tablet contains: Suvarna Vasant Malati 1.5 mg. Talispatra (Taxus Baccata) 30.0 mg. Asan (Withania somnifera) 30.0 mg. Abhrak Bhasma (Mica Bhasma) 15.0 mg. Pravala Bhasma (Corallium rubrum) 30.0 mg. Svarnamakshika Bhasma (Ferri Sul-phuratum) 15.0 mg. Ardusi Ghan (Adhatoda Vasica) 15.0 mg. Amala (Emblica Officinalis) 30.0 mg. Galo (Tinospora cordifolia) 30.0 mg. Dagdi Pashan Bhed (Saxifruga ligulata) 30.0 mg. Pipar (Piper longum) 30.0 mg Kachura (Curcuma Zedoaria) 30.0 mg. Ardusi (Adhatoda vasica) 15.0 mg. Shatavari (Asparagus recemosus) 30.0 mg.
MATERIALS & METHODS
In this study Dekofcyn was tried in 60 chil-dren aged between 1 year and 8 years. All were suffering from cough of moderate to severe in-tensity. Dekofcyn was given for a period of 2 weeks to 2 months in a dose of 1 tablet two times a day or three times a day, depending upon the severity of cough and the age of the child. Where there was complete relief, Dekof-cyn was continued for one more month in a maintenance dose of 1 tab. two times a day.
The following investigations were done wherever possible: C. B. C., E. S. R., Screening of the chest, Mantoux Text (MT), and stool examination.
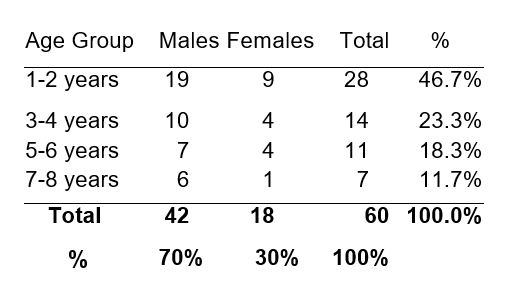
AGE GROUPS The largest number of children, namely 28 (46.7%) were in the age group of 1-2 years. There were 42 male children (70%) and 18 female children (30%). More male children are in our series, probably because more care is generally taken of the male child than the female child in our Indian society, though the incidence of respiratory diseases and cough is the same in both sexes of children.
TABLE-I
Age Groups & Sex
DURATION OF COUGH About half the number of children had cough ranging from 15 days to 3 months and the other children had cough ranging from 4 months to 12 months, off and on.
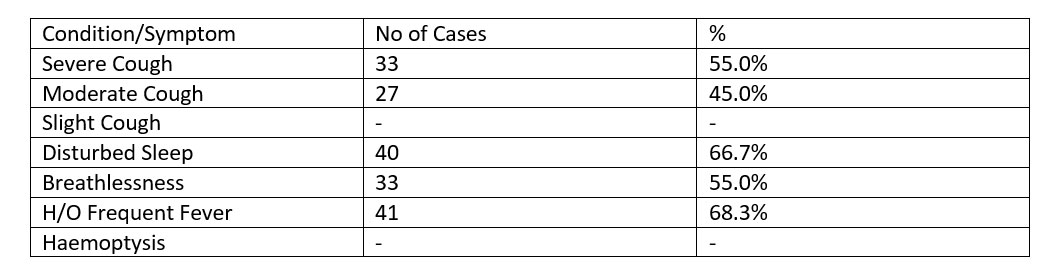
SYMPTOMS Each child had one or more than one symptom. All children were suffering from cough of moderate to severe intensity. 40 chil-dren (66.7%) had disturbed sleep due to cough and 33 children (55%) had breathlessness. History of frequent fever was present in 41 chil-dren (68.3%). There was no case of haemoptysis in our series. (Table II).
TABLE II SYMPTOMS: NO = 60
|
|
INVESTIGATIONS
Blood examination (CBC), ESR, examination of stools, Screening and Mantoux Test (MT) were done.
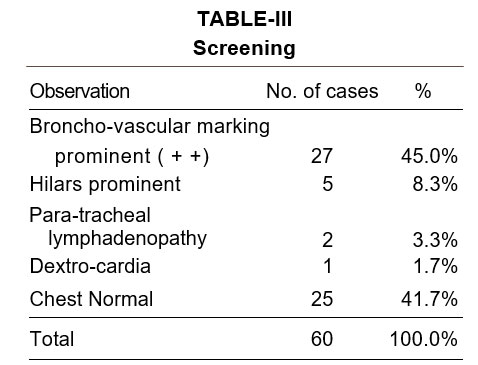
SCREENING
Screening was done in all children. 27 children (45.0%) had prominent Broncho-vascular markings + +, 5 children (8.3%) had Hilars Prominent, 2 children (3.3%) had para-trachial lymphadenopathy, and one child had dextrocardia. Chest was normal in 25 children (41.7%) (Table III)
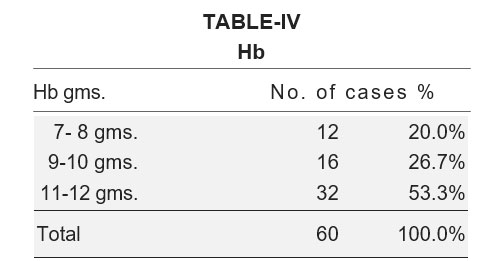
22 children showed higher WBC count and 10 children showed more than normal eosinophil count ranging from 9.20%. Hb values are given in Table IV.
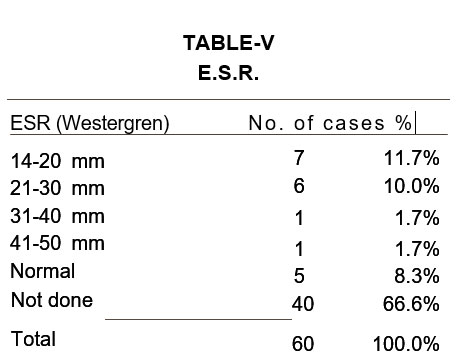
ESR was done in 20 cases. The value was 14-20 mm in 7 children (11.7%), 21-30 mm in 6 children (10.0%), 31-40 mm in one child (1.7%), 41-50 mm in one child (1.7%) and it was normal in 5 children (8.3%). ESR was not done in 40 children (66.6%). (Table V).
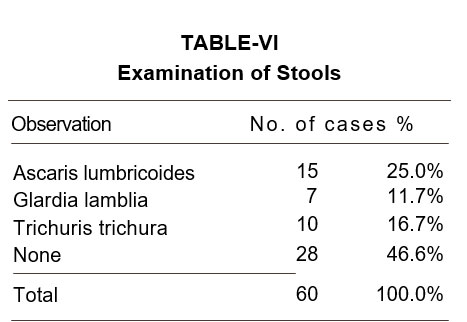
EXAMINATION OF STOOLS
Stools were examined in all 60 children.15 children (25%) had Ascaris lumbricoides. 7 children (11.7%) had Giardia lambia and 10 children (16.7%) had Trichuris Trichura. 28 children (46.6%) showed no infestation of worms. (Table VI).
MANTOUX TEST (MT)
Mt was done in all children. It was positive only in 2 children, and in other it was either within normal limits or negative.
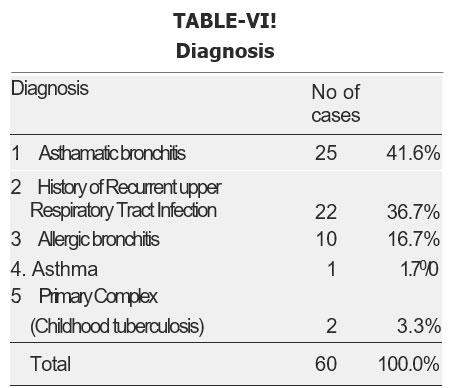
DIAGNOSIS
There were 25 cases of asthmatic bronchitis, 22 cases with history of recurrent upper respiratory tract infections, 10 cases of allergic bronchitis, one case of asthma and 2 cases of Primary Complex. (Table VII).
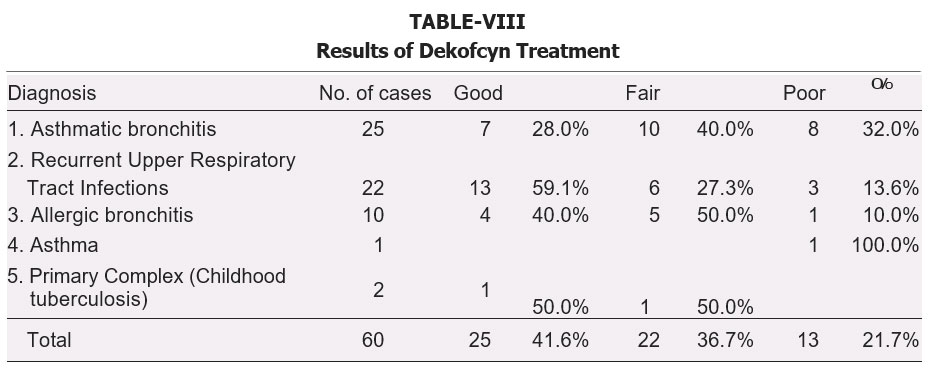
RESULTS OF DEKOFCYN THERAPY
Results were classified as Good when there was complete relief of cough in cases of Recurrent U.R.T. Infections within one to two weeks and in cases of chronic types of cough within one or two months of Dekofcyn therapy. On this basis, the results were classified as Good, Fair, or Poor. However, Dekofcyn was continued in a dose of 1 tab. two times a day, for one month, in all cases, as a maintenance dose.
There was Good relief of cough in children of asthmatic bronchitis, 13 children of Recurrent URT infection, 4 children of allergic bronchitis and in one child of Primary complex. There was Fair response in 10 children of asthmatic bronchitis, 6 children of Recurrent URT infections, 5 children of allergic bronchitis and one child of Primary Complex. The response was Poor in 8 cases of asthmatic bronchitis, 3 cases of Recurrent URT Infection, 1 case of allergic bronchitis and in 1 case of asthma. Overall response among 60 children treated with Dekofcyn was that 25 children (41.6%) had good relief, 22 children (36.7%) had Fair Relief and 13 children (21.7%) had Poor Relief. On the whole 47 children (78.3%) had satisfactory relief from cough with Dekofcyn treatment. (Table VIII).
DISCUSSION & SUMMARY
Cough being a troublesome and distressing symptom causes disturbed sleep in many children. In this series, 66.7% of children had disturb sleep. Most of the children had wheezing, 20 children (33.3%) had associated congestion of throat, 33 children (55%) had breathless-
ness, and 10 children (16.7%) had severe rhinitis. One child had local epilepsy following meningeal infection. After Dekofcyn therapy, the children had less disturbed sleep and had good relief from wheezing and breathlessness. Weight gain was evident in many children and though this could not be attributed to Dekofcyn
therapy directly, it was an indication of the general well being of the child following the relief of cough and associated symptoms. Repeat examinations of blood etc. were done wherever necessary. No side effects were observed with Dekofcyn treatment.
From this clinical trial it is observed that De-kofcyn is a safe and beneficial drug in the man-agement of cough in children.
ACKNOWLEDGEMENT
I express my thanks to Alarsin Pharmaceuti-cals, Bombay-400 023, for their co-operations. REFERENCES 1. Chaudhari S. N. Das: Antitussive Effect of T. Tone (Dekofcyn) in cougs of Tubercular Ori-gin; Cur. Med. Pract., Vol. 19: 3; 119-23, Mar. 1975.
2. Deshpande Arun D. & Wagh V. M.: Pilot Study of T. Tone (Dekofcyn) in Bronchiec-tasis — World Cong. on Asthma, Bronchitis & conditions allied, New Delhi, Nov. 74 & Mah. Med. Jr., Vol., XXIII, No. 12, March 1977.
3. Gupta, J._P.: T. Tone (Dekofcyn) in various forms of Pulmonary conditions — The Jr. of Chikitsak-Parishad, Vol. II, No. 3, Mar. 1971.
4. Joshi V. S. & Jyoti Aholkar: Dekofcyn for cough in Infants & Children — Medicine & Surgery, Vol. No. 12, 22-25, Dec. 1977.
5. Kale, Madhav K. Double-Blind trial of Dekof-cyn to assess its usefulness in cough and other symptoms in cases of pulmonary tuberculosis: Mediscope, Vol. XX, No. 11, 241-47, Feb. 1978.
6. Mathur, J.B.L., Cough in Pulmonary Tuber-culosis (A Clinical Study with Ayurvedic Drug T. Tone — (Dekofcyn), Indian Pract. Vol. XX, No. 6 June 67. 1977.
7. Shah B. N., A Talispatra (Taxus Baccata) Compound (Dekofcyn in cough of Pulmo-nary Tuberculosis (A Clinical Study of Hos-pitalised patients): 41st All India Med. Conf., Baroda, Dec. 65 & Patna Jr. of Med. Vor. 40, No. 3, March 1966.
8. Sharma D.D., Study of an Ayurvedic Drug T. Tone (Dekofcyn) in control of cough in tuberculosis — Mah Med. Jr., 21 : 11. Feb. 1975.
9. Shrimankar, J.N., Mohanty, K.C. & Master, T.B., Antitussive effect of T. Tone (Dekof-cyn) on Chronic cough — Cur. Med. Pract. Jul. 75, Vol. 19, No. 7, 1975.
10. Vakil, P.R., An Ayurvedic “Antitussive” (Dekofcyn) (A Clinical Study) — The Indian Pract. 17:12, Dec. 1974.